THE CELLULAR BATTERY // CREATINE MONOHYDRATE
Creatine is the most-studied, cheapest, and most misunderstood molecule in the performance world. It is not a stimulant or a hormone — it is a rechargeable battery. Your cells store it as phosphocreatine and draw on it to regenerate ATP in the first seconds of any hard effort, muscular or mental. The muscle case is closed: across decades of randomized trials, creatine plus resistance training builds more strength, more lean mass, and better physical function than training alone — and the effect holds into old age, exactly when it matters most (Devries et al., 2014). The brain case is more interesting and more honest: creatine measurably helps cognition, but mainly where brain energy is under strain — aging, sleep deprivation, a plant-based diet — and barely at all in a rested young omnivore (Xu et al., 2024; Sandkühler et al., 2023). And the reputation that keeps sensible people off it — that it wrecks your kidneys — is a myth built on a lab artifact; controlled trials find no renal harm at normal doses (Longobardi et al., 2023). A rare case where the ruler rewards: proven, cheap, safe. The only discipline required is telling what it does from what it is sold as.
Creatine sits at an unusual intersection: it is at once the most-researched sports supplement in existence and one of the most misunderstood. Two myths bracket it. The first oversells — that it is a general-purpose 'smart drug.' The second undersells — that it damages the kidneys. Both are wrong, and the truth between them is better than either.
The mechanism is not exotic. Creatine is stored as phosphocreatine, a high-energy phosphate reservoir the cell taps to regenerate ATP faster than metabolism alone can manage. Muscle draws on it in the first seconds of a hard set; the brain draws on it during intense or energy-starved cognition. Supplementation raises those stores. That single fact is the basis of every real effect — and the reason the effects surface most where the battery is most drained.
We grade creatine CLINICAL because the muscle and safety evidence is genuinely closed. We also refuse to let that grade launder the cognitive claims, which are real but conditional. Proven where it is proven. Calibrated where it is not.
The Muscle Case — ClosedTIER A
Meta-analyses spanning hundreds of participants show creatine plus resistance training produces greater gains in fat-free mass and strength — chest press, leg press — than resistance training alone, with better performance on functional tests such as the 30-second chair stand (Devries et al., Medicine & Science in Sports & Exercise 2014). The effect is not confined to the young: in older adults, adding creatine to training augments lean tissue and lower-limb strength, with benefits accruing over roughly 8-32 weeks (Liu et al., European Review of Aging and Physical Activity 2025; Santos et al., Nutrients 2021). For a population losing muscle to age, that is a rare, cheap, evidence-backed countermeasure.
Creatine does not build muscle on its own. It lets you do slightly more work, recover slightly faster, and hold more substrate inside the cell — and those small margins compound across months of training. Remove the training stimulus and the effect shrinks toward nothing. It is an amplifier of work, never a substitute for it. This is the cleanest line in the whole file: the supplement is real, the barbell is still mandatory.
The Brain Case — Real, But ConditionalTIER A (CONDITIONAL) / TIER B (MOOD)
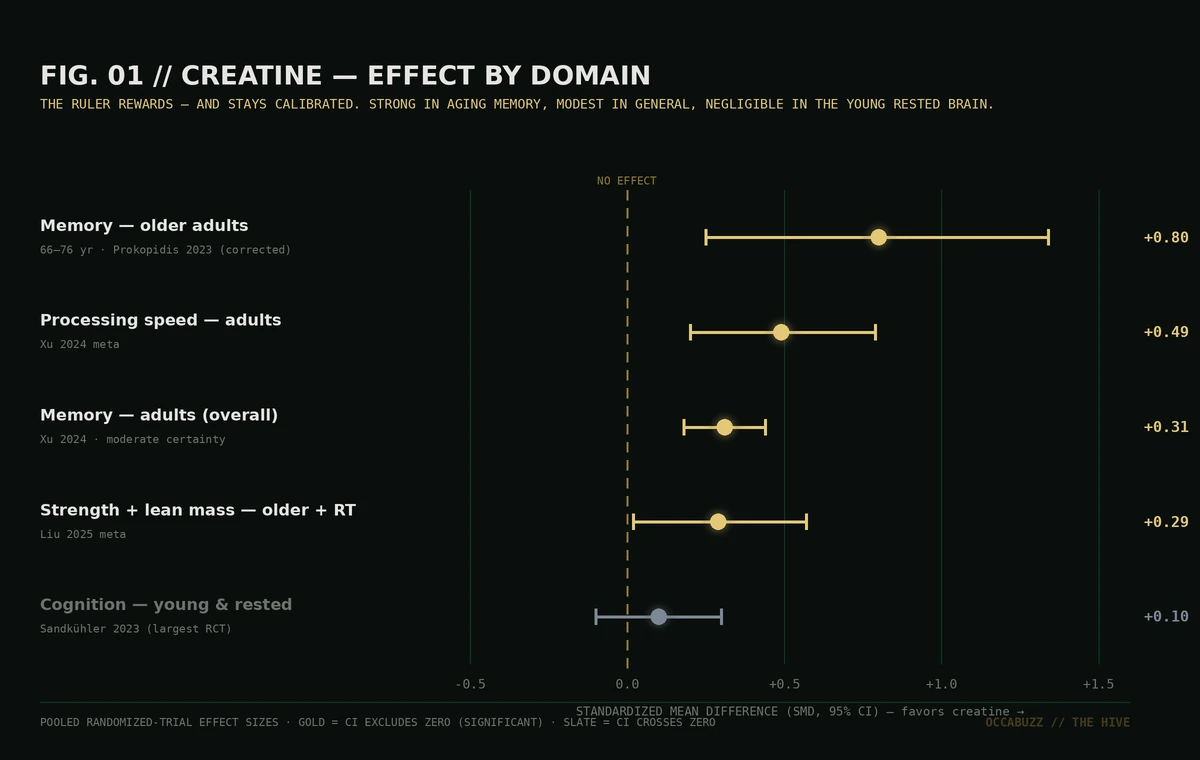
A 2024 meta-analysis of 16 RCTs found creatine significantly improved memory, attention, and processing speed — with moderate GRADE certainty for memory — and larger effects in older and clinical populations (Xu et al., Frontiers in Nutrition 2024). The aging signal is the strongest. After a statistical correction to an earlier meta-analysis, the overall memory effect in the general population fell to non-significant, but the benefit in adults aged 66-76 held firmly (SMD 0.80; Prokopidis et al., corrected 2023). Under acute sleep deprivation, a single high dose (0.35 g/kg) improved cognition and restored brain high-energy phosphates on 31P-MRS (Gordji-Nejad et al., Scientific Reports 2024).
The largest cognition trial to date is the discipline. In 123 mostly young, rested adults taking 5 g/day for six weeks, creatine produced only a small, borderline effect — and, tellingly, vegetarians did not benefit more than omnivores (Sandkühler et al., BMC Medicine 2023). The pattern across the literature is consistent: creatine helps the brain when the brain is energy-stressed. A rested twenty-five-year-old is not energy-stressed, and should not expect the aging-memory result to be theirs.
As an add-on, creatine shows early promise in depression: 6 g/day alongside cognitive-behavioural therapy beat CBT plus placebo over eight weeks (PHQ-9 −5.12; Sherpa et al., European Neuropsychopharmacology 2024), and a 2026 systematic review found a signal for creatine augmenting SSRIs or psychotherapy in major depression. It is an adjunct, not a treatment — and in bipolar illness two trial participants switched into hypomania, so it is not casual self-medication.
Is creatine a proven longevity-and-cognition tool — or a muscle supplement the internet reinvented as a brain drug?
Decades of randomized trials. Creatine plus training beats training alone for lean mass, strength, and function — into old age. This part is not in dispute, and it is the core reason to take it.
Devries et al. — Creatine + resistance training in older adults: meta-analysis (Med Sci Sports Exerc, 2014) ↗Real gains in memory and processing speed — concentrated in aging, sleep loss, and plant-based diets. In the young and rested, the effect is small at best. Bank on it selectively, not universally.
Xu et al. — Creatine & cognition: systematic review & meta-analysis (Frontiers in Nutrition, 2024) ↗The most persistent reason people avoid creatine is the least supported. Controlled trials show no renal harm at recommended doses; the rise in serum creatinine is the molecule metabolizing, not the kidney failing.
Longobardi et al. — Requiem for creatine-induced kidney failure? A narrative review (Nutrients, 2023) ↗The honest synthesis: creatine is one of the few supplements where the evidence is strong enough to be boring. For muscle and strength — especially with training, especially with age — it works, cheaply and safely. For cognition it works too, but selectively: bank on it if you are older, sleep-deprived, or plant-based; do not if you are a rested young omnivore expecting a nootropic. And the kidney fear that keeps sensible people away is a misread lab value, not a hazard. Proven, calibrated, and about forty cents a day.
Creatine is one of the rare cases where the baseline is the intervention: 3-5 g of monohydrate a day, paired with the training and sleep that do the heavy lifting. It amplifies a stimulus; it does not create one. Lift, and it builds more muscle than lifting alone. Sleep badly, and a larger dose softens the cognitive hit — but fixing the sleep beats dosing around it. Eat little meat, and it refills a store your diet keeps low. There is no exotic protocol to buy: the monohydrate is the whole product, and everything premium-priced past it is solving a problem you do not have.
If you acquire creatine through our vetted links we may earn an affiliate commission — at zero cost to your capital — and it changes nothing here. Creatine is cheap enough that there is little margin to distort; we grade it CLINICAL because the muscle and safety evidence is closed, and we hold the cognitive claims to 'conditional' precisely because the market wants us to round them up. Buy plain monohydrate. The evidence drives the grade. Nothing else does.